If you’ve been following this blog for any amount of time, you know how passionate I am about heart disease screening. I’ve released numerous podcast episodes on the subject of heart disease screening, which have gotten a lot of interest over the years.
That tells me I’m not the only one excited about this topic.
Heart disease is the number one killer of humans in the U.S. and on the planet. If you’re prioritizing longevity in your health journey, few things are more important than heart screening as a tool for avoiding that statistic.
To that end, I want to dive a little deeper into a revolutionary piece of technology that’s changing how we evaluate cardiovascular risk, how we stratify it, and how it impacts heart disease outcomes.
Heart Screening the Old Way
Before the technology I’m discussing entered the picture, the standard for cardiovascular risk stratification — how we evaluate and identify heart disease — was based on population health, or what’s best for the population as a whole.
In theory, this is great. Population health looks at an enormous group of people, extrapolates the most dangerous scenarios amongst that group — in this case for heart health — and applies them to everyone else. The powers that be then develop heart screening tools to catch those big risk factors in patients’ routine medical care.
This acts as a kind of sieve for all patients to pass through. If you start showing some of the most common signs of heart disease, the sieve “catches” you. In other words, you register as “at risk” in the population health paradigm.
A whole range of factors are currently considered in heart disease screening. For instance:
- Do you have high blood pressure or high cholesterol?
- Do you lead a sedentary lifestyle?
- Do you have a family history of heart disease?
Patients generally follow a path of annual heart screenings to detect high blood pressure, high cholesterol, diabetes, and other “classic” symptoms like chest pain and shortness of breath. From a population health standpoint, these symptoms indicate heart disease is present.
While this approach is certainly better than nothing, it unfortunately falls short in two important ways:
- Once the symptoms these heart screening tests look for appear, heart disease is already advanced enough to cause symptoms!
- These heart screenings fail to identify those who have early heart disease and who, by definition, aren’t yet showing symptoms.
A lack of heart disease symptoms doesn’t equate to a lack of heart disease. In fact, that’s the time we really want to identify whether you’re moving toward future cardiovascular issues — so we can attack the problem before symptoms appear, while there’s still time to reverse course.
The Gaps in Traditional Heart Screening
Let’s look at the experience of a 55-year-old man with a moderate risk profile.
This man is 50 pounds overweight. He has high blood pressure, high cholesterol, and a family history of heart disease. But he works out vigorously four days a week, and he has no chest pain or shortness of breath to speak of.
This man might consider himself a bit overweight and a bit short of his ideal health. He’s getting concerned because his dad had a heart attack around this age.
At his annual wellness visit, his doctor orders a stress test, but because this patient exercises regularly with no symptoms, the test comes back negative (no surprise there). He has high blood pressure, and his blood work shows high cholesterol, but that’s nothing a little medication can’t fix. He’s also noted to have “borderline” diabetes.
The doctor’s conclusion? “Eat a little less, exercise a little more, take your medications, and we’ll reevaluate in a year.”
Three months later, the patient winds up in the ER suffering from a heart attack. This is the same man who left his annual checkup with no heart disease diagnosis!
There’s a huge disconnect between the individual symptoms you might exhibit and the conditions you actually have. It’s almost a universal experience: You’re fine until you’re not.
Heart Screening: Why Symptoms Aren’t Enough
What most people don’t understand is that in traditional healthcare, the main — if not the only — metric used to gauge whether an intervention is needed is a person’s symptoms. The problem with that approach is that symptoms only appear at the end of a disease cycle. In other words, symptoms are a late finding.
In most instances of chest pain and shortness of breath, you won’t notice something’s wrong until you have a blood vessel that’s over 90% blocked. Moreover, even if your heart vessels are incredibly blocked and you have profound heart disease, you might not exhibit a single symptom.
We as physicians have been asking (and answering) the wrong questions. When we conclude you don’t have symptoms, we’re only confirming you’re likely not at a disease’s end stage.
What we need to ask instead is, How much disease is present? When you’re overweight, 55 years old, have a family history of heart attacks, and have diabetes and hypertension, it’s unlikely you don’t have heart disease. With those conditions, it’s almost completely impossible not to have any atherosclerosis!
Here’s an analogy I like to use: You can get an oil change and tire rotation on your car every 5,000 miles with no check engine light, but just because you get that service regularly doesn’t mean it’s impossible for your check engine light to turn on.
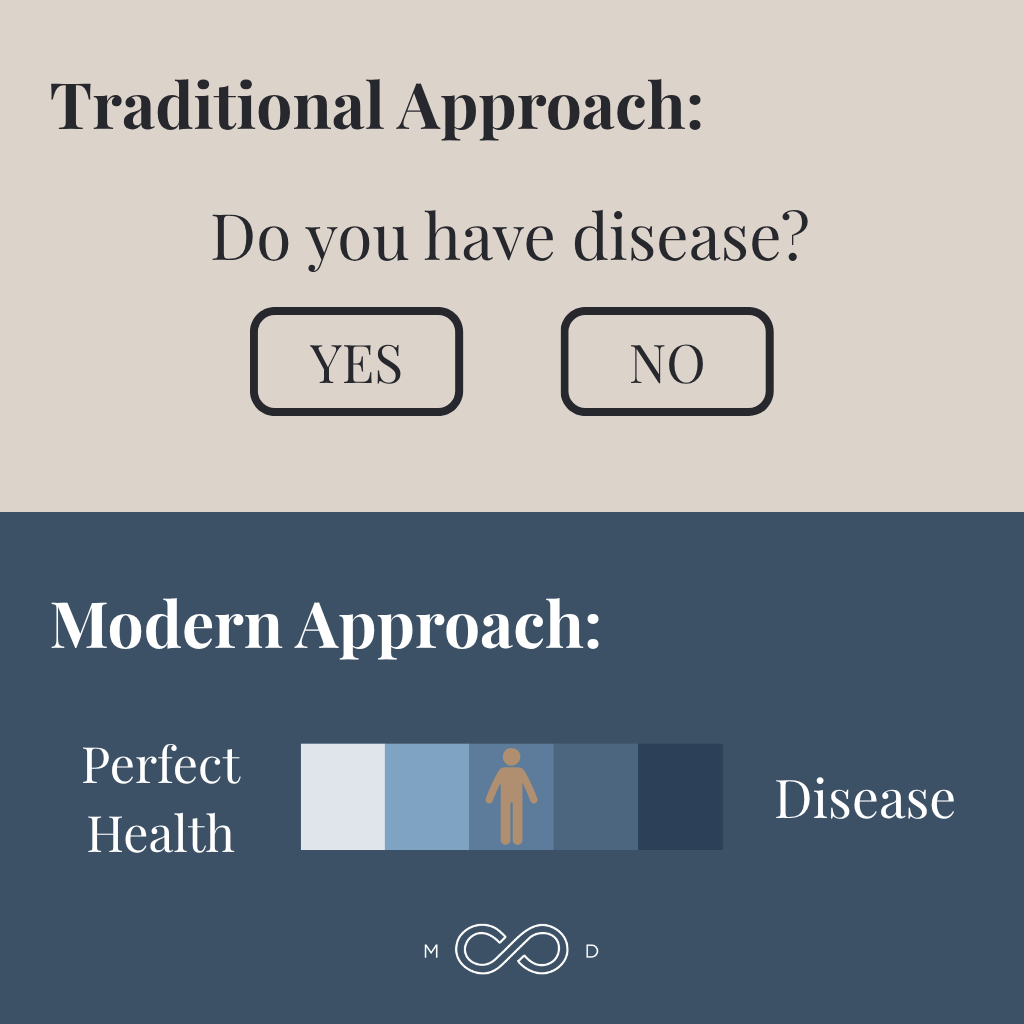
In our current healthcare model, there’s no pathway for intervention before bad outcomes happen. We’re part of a reactionary system, and it’s a borderline approach we’ve discussed in the past.
While many healthcare providers don’t fundamentally believe diseases are binary, most patients are managed as if they either have a condition or they don’t. Most diseases, including heart disease, fall on a spectrum our current paradigm doesn’t address.
This isn’t due to a lack of trying. Many doctors would love to actively prevent disease, but they simply don’t have the tools, the time, or the permission from insurance companies or administrations to dig deeper.
If patients need the bulk of their costs covered through health insurance, for instance, newer or more advanced heart screening tests may run outside the scope of their coverage — because health insurance only pays based on population health-based recommendations. If a doctor has a feeling they should dig deeper into a patient’s health but the patient has no way to pay for that digging, there’s nothing they can do.
In short, there hasn’t been a better way to screen for heart disease. Until now.
Cleerly for Heart Screening: What It Is and Why It’s Useful
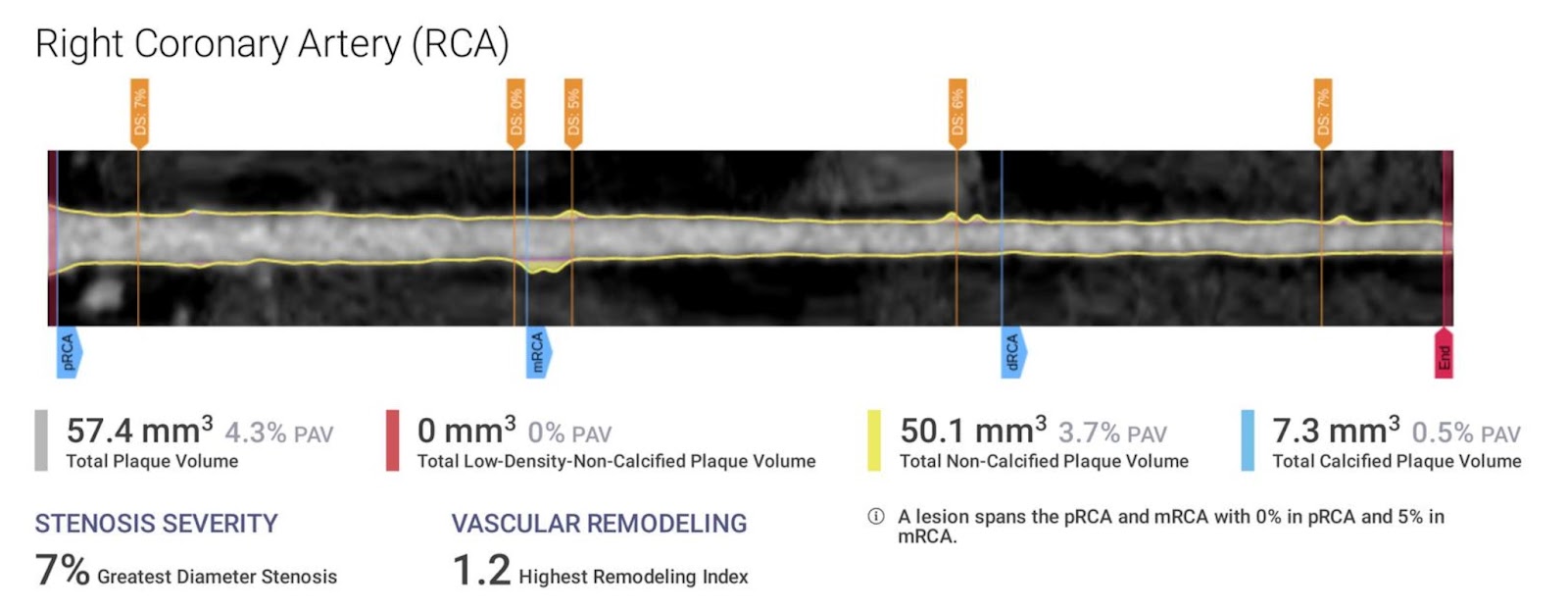
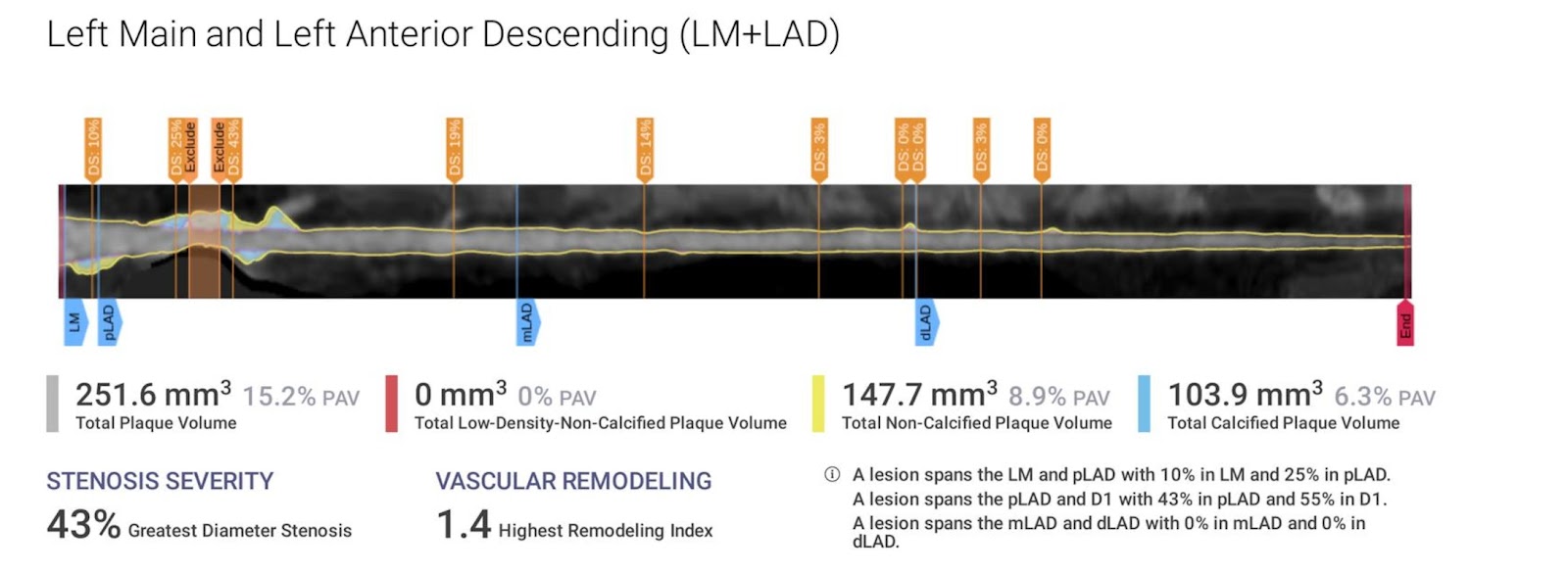
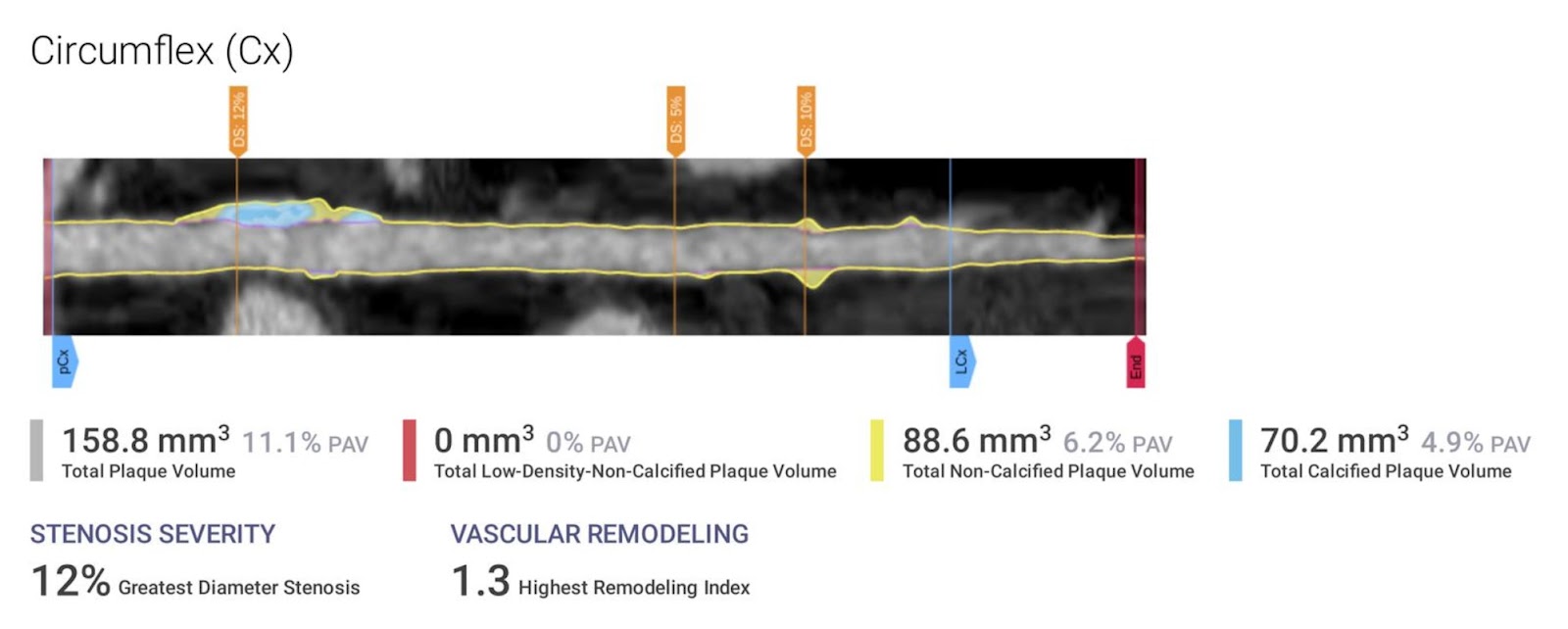
A relatively new healthcare technology company called Cleerly has harnessed the power of artificial intelligence to take high-resolution pictures of the coronary arteries. These arteries funnel oxygenated blood to the heart — and they’re also where plaques form and heart attacks happen.
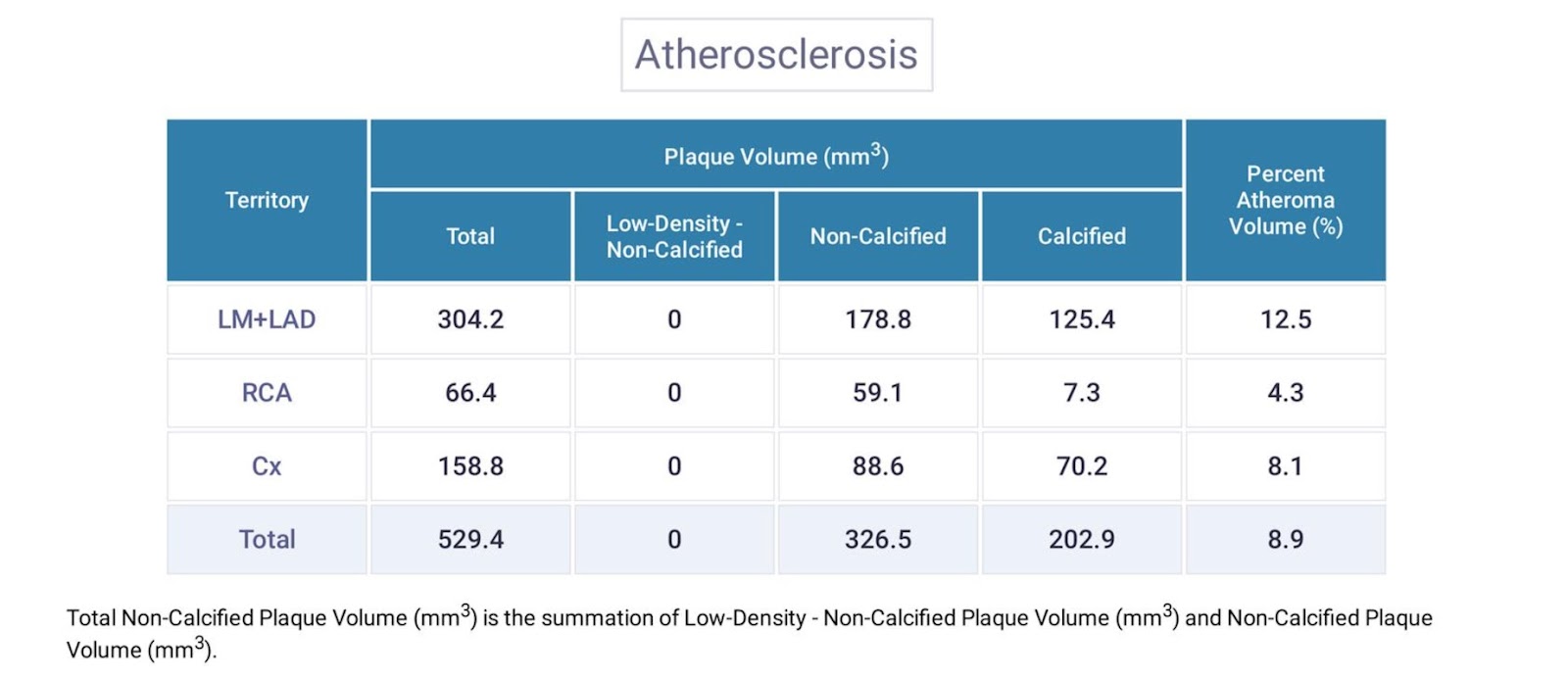
Cleerly extracts from these pictures granular data about the nature and amount of plaque in the coronary arteries. It can measure in grams the cumulative total plaque burden on your heart, and it can give a segmented analysis of each coronary artery and its unique contribution to that plaque burden.
Why Is Plaque So Important?
Plaques, or fatty deposits, build up in the arteries in response to various stimuli, such as inflammation. Over time, this plaque hardens, or calcifies, to cause atherosclerosis. Until Cleerly, the only routine heart screening we had to evaluate plaque buildup in the arteries was called a calcium score, a test which exclusively detects this calcified plaque.
But calcified plaque isn’t the only plaque. Before they calcify, plaques are soft and unstable, and they can rupture. When a plaque ruptures, a blood clot forms, breaks away from the inside lining of the artery, and travels with the blood flow downstream into a smaller artery.
If that clot gets stuck in a smaller artery, it’s like a big boulder in a creek, stopping all downstream flow of oxygenated blood through that channel, killing the heart cells that should be fed with that blood flow. That’s what creates the chest pain we know as a heart attack — dying heart cells.
What Is Cleerly’s Role in Diagnostics?
Previously, the only way to get an idea of someone’s soft plaque buildup was through a heart catheterization, an invasive procedure in which dye and a catheter are inserted into an artery to take pictures.
The new technology from Cleerly is changing the game. Now, we can see not only the quantity and location of plaque buildup, but we can also get an idea of what type of plaque it is (stable or unstable) without a heart cath procedure.
What Are the Benefits of Detection and Prevention?
Most heart attacks happen because of these small, noncalcified, unstable plaques. In the past, we’ve often thought of heart attacks as most often stemming from a big mountain of plaque blocking an artery, especially when that plaque is predominately calcified, stable plaque.
We’re now learning that it’s the smaller buildups that cause many heart attacks. These may cause less than a 50% blockage, but they’re completely unstable and prone to rupture.
Cleerly is incredibly powerful because it identifies the location and composition of the plaques in question — that is, are they calcified or noncalcified, stable or unstable — which can drastically change your treatment plan.
When you get this heart screening as a baseline and find a problem, you as the patient now have the power to repeat the test annually to evaluate your treatment effectiveness. You get to see if the composition, not just the quantity, of your plaque changes over time.
In a lot of ways, this approach can help you avoid heart attacks because you’ll see them heading toward you from quite a distance. If you find a concerning, unstable plaque early, you can potentially manage its composition and render it less dangerous. You can intervene before escalating plaque becomes a problem.
Cleerly in an Unclear System: Heart Screening Challenges
Despite its advantages, Cleerly isn’t yet part of the population-health model, so there may be challenges with getting this heart screening for yourself. Some of the issues at the time of this writing include:
Accessibility
A challenge that comes with any groundbreaking revolutionary technology is that it’s not widely available. In many places, the first challenge will be finding a CT machine that can support a Cleerly study.
Perhaps surprisingly, not all CT machines are created equal. Brentwood MD operates in the greater Nashville market, and even this busy area has only one CT machine (so far) that produces the high-quality images required to use Cleerly technology.
You might say, “Why wouldn’t everyone have the best-of-the-best equipment now that it’s out there?” Unfortunately, it’s because these machines cost millions of dollars, and institutions have to justify the costs of their investments to all kinds of parties. A “serviceable” but cheaper CT machine may be all a facility can get approved to purchase.
Ordering the Test
A second factor is that you need to find a cardiologist who knows about the Cleerly test and has the ability and willingness to order it. Not all cardiologists know about Cleerly or are convinced of its benefit. This is where finding a healthcare team aligned with your goals is crucial.
At Brentwood MD, we’re fortunate to have built a relationship with Cleerly, but we only have that relationship because we took the initiative to create it. Look for a provider who is willing to do the same.
Cost
The last challenge to overcome is Cleerly’s cost. If you’re dependent on insurance to pay for heart screening and don’t have a clear medical narrative that indicates you need this test, you may be forced to pay for the service out of pocket or look into alternative testing.
It can cost several thousand dollars to perform this heart screening, and access to an adequate CT machine is a real barrier. At Brentwood MD, we’re fortunate to have negotiated very favorable rates for those who don’t use insurance. Still, as of now, this particular heart screening is a real investment, one not everybody has the capacity to make.
On the positive side, Medicare has been considering adding Cleerly testing to its coverage, so be sure to check if this applies to you!
Still, with the barriers above in mind, it’s no wonder many cardiologists aren’t yet enthusiastic about ordering a Cleerly test in the absence of chest pain or shortness of breath. If patients don’t have symptoms, it’s unlikely insurance is going to get involved. With that said, I haven’t had a patient who couldn’t get insurance to cover Cleerly if their situation warranted it.
Cleerly: The Modern Heart Screening We’ve Needed
Here at Brentwood MD, we’re extremely passionate about Cleerly. Not only is this technology incredible, but it fits quite well into our mission of helping you live a long time and feel great doing it.
If you have the means, I can’t think of a better place for investing some discretionary income than up-to-date heart screening. Cleerly offers an unprecedented opportunity to get meaningful data on the number one disease most likely to take every human being off this planet — especially if you have a high-risk profile. Among health pitfalls to hunt for, heart disease needs to be at the top of your list.
If you want to know more about Cleerly, visit their website for more information.

Dr. Aaron Wenzel is a concierge physician specializing in the care of fast-moving entrepreneurs, executives, and public figures in the Nashville, TN area. Dr. Wenzel’s diverse life experience and extensive training in family medicine, emergency care, nutrition, and hormone replacement therapies give him the unique platform to provide unmatched care for his patients.